12July, 2023
Adenomyosis and Infertility
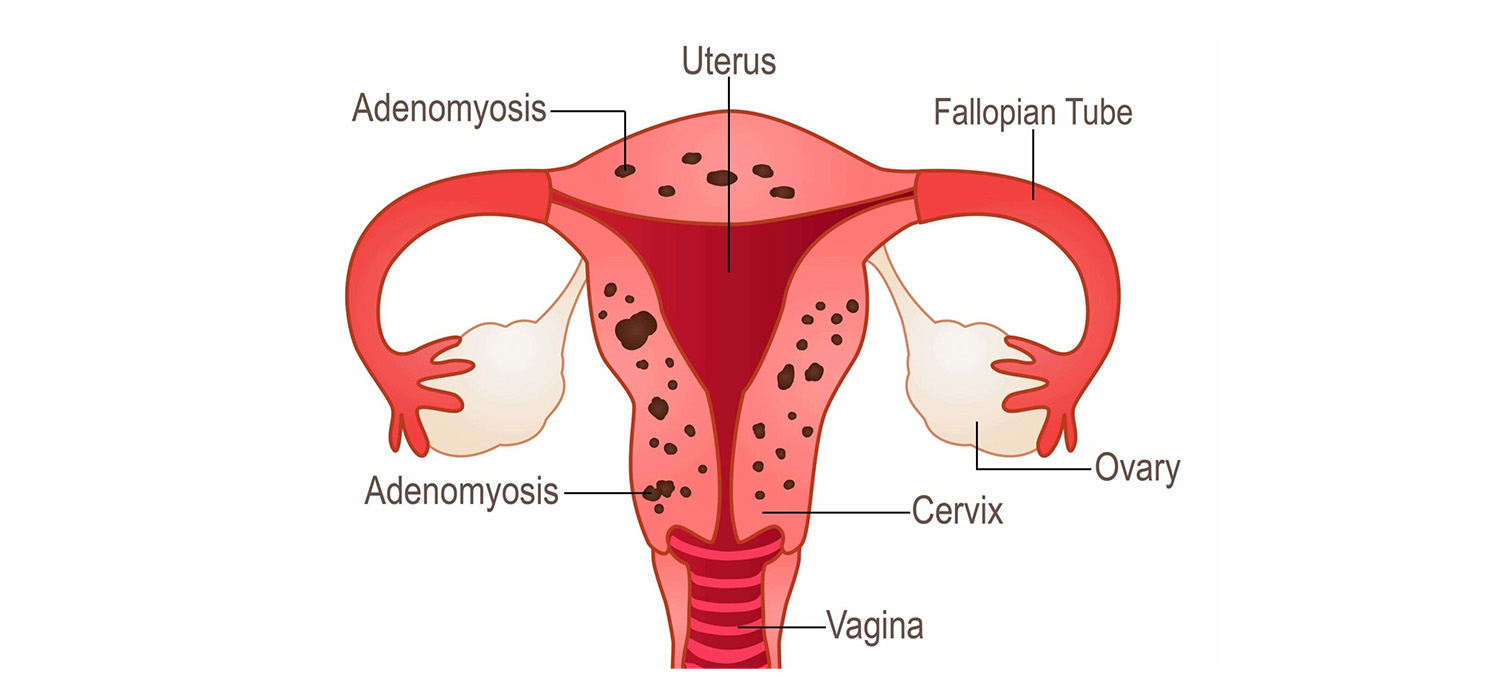
Adenomyosis is the presence of endometrial stroma and glands within the myometrium. The prevalence is around 20% in young girls and about 32% in women between 42 and 49.
Symptoms include dysmenorrhoea, menorrhagia, pelvic pain and infertility.
Pathogenesis of adenomyosis
It is believed that polymorphism in ER-α gene confers the risk of developing endometriosis. The adenomyotic tissue within the myometrium has increased number of steroid receptors and has excessive aromatase and sulphatase activity. The latter two cause conversion of Estrone-3-sulphate into estrone which then acts on estrogen receptors and causes f=growth of the adenomyotic tissue.
Also reduced progesterone receptors in the adenomyotic tissue promotes the development and progression of adenomyotic tissue.
Diagnosis of adenomyosis
Transvaginal scan and MRI can diagnose adenomyosis. MRI has greater accuracy and can assess JZ thickness and extent of myometrial involvement. Definitive diagnosis is by histopathological examination of the adenomyotic tissue.
Effect of adenomyosis on IVF
Adenomyosis is associated with reduced fertility and low success with ART. Reduced response to ovarian stimulation, reduced implantation and clinical pregnancy rates, increased miscarriage rates and reduced live birth rates are observed in women with adenomyosis.
Medical management of adenomyosis
The objective of therapy is pain relief, to reduce menstrual flow and to improve fertility. The underlying principle is to reduce the production of endogenous estrogens or induce endometrial differentiation with progestins.
Non-hormonal medical therapies include pro-coagulant agents, NSAID, Iron supplements. Hormonal treatment are GnRHa, Progestins and COCs.
Progestins act by causing decidualization and atrophy of endometrial tissue; modulation of mitotic activity/local growth factors & receptors and also via paracrine and anti-inflammatory mechanisms. Nor ethisterone acetate, Dienogest and LKG-IUS are some of the medications in this category. Danazol is not used for its unacceptable side effects of virilization.
GnRHa alleviates the symptoms by reducing the gonadotrophin secretion and steroidogenesis. Long acting GnRHa is used in ART for downregulation. Hypoestrogenic state is the common side effect and can be overcome with add back estrogen therapy.
COCs reduce aromatase expression and by causing decidualization and atrophy of endometrium, reduce the menstrual flow. They can only be used for reducing the symptoms and not for fertility treatment for obvious reasons.
Other drugs that are being tried for therapy include aromatase inhibitors that act by reducing estrogen synthesis. SERMs and SPRMs are the new group of drugs being tried and more RCTs are needed.
Surgical treatment of adenomyosis
This is beneficial for those with previous IVF failures and increases spontaneous pregnancies.
Localized adenomyosis can be removed by lap excision or Robotic assisted surgery. Adenomyosis which is mainly sub-endometriotic, that is less than 2.5 cms deep from the surface, requires hysteroscopic resection. Diffuse adenomyosis merits prolonged treatment and has poor results with ART. HIFU and HIFU-Mrg are experimental.
Management for ART
Pooling cycles followed by FET can be done. Ulipristal acetate for one or two courses, three months apart has been tried prior to ART. But more studies are needed. Surrogacy may be offered for multiple failed IVFs.
For more info, Visit : www.medlineacademics.com